
COVID-19 Chat
MOUnt Sinai
TLDR:
Role:
UX Design Lead
Team:
Design Lead, Product Manager, 2 Developers
Duration:
March 2020 - Ongoing
Methods:
Flow Diagramming
Service Design
Hi-fi Design
Stakeholder Management
Main Stakeholder
Mount Sinai Health System
This was a health system-wide initiative to respond to the dramatic increase in need patient care and attention during the COVID-19 crisis in NYC.
Problem Space
Mount Sinai has one of the largest hospitals in the US, in a city hardest hit by COVID-19.
We have to be able to effectively help the general public with their health concerns, while balancing the resource constraints our frontline health workers face daily. At NYC’s COVID height in late March and early April, Mount Sinai’s hospitals were buckling under the weight of in-person visits to the system and our emergency departments. To best protect both our patients and our staff, we needed to create a solution to help triage patients to the best outcome for their needs, quickly.
Solution
COVID-19 chatbot and live chat step up.
Creating a chatbot solution that triages patients to the resources they need while making sure that medical professionals are able to connect with the patients in most critical need.
Solution
We created automated chatbot logic to help patients assess their symptoms with 3 main possible resolutions:
-
Health system endorsed (i.e. trusted) online COVID resources;
-
Entering a video based, urgent care services;
-
Live chatting with a registered nurse on staff.
Sample flow taken from live product displayed below. This is not a comprehensive demo:
The goals
-
Creating a chatbot solution that triages patients to the resources they need while making sure that medical professionals are able to see the patients with the most critical need.
-
Create something that was technically flexible and made updates easy. Speed was of the essence given the daily changes to what we knew about the virus and also ever changing hospital resources.
The process
It started the first week of March when I returned from Seattle (just before it was about to become the first coronavirus hotspot). Over the course of 1 week in fact and we had to use what we already had, but make an experience that could handle a significant, sustained amount of volume. The most important piece here was clarity upfront of what we were trying to achieve.
My product manager and I worked hand in hand to create an experience using our existing chatbot functionality (up until this point had only been used for triaging low-risk seasonal flu patients and self-scheduling appointments). Though the chat experience has been (and remains) imperfect, it was the optimal solution for a few reasons:
-
Mobile accessibility: According to Pew Research, amongst lower income households, 71% have access to a smartphone, but only 54% have access to a laptop or desktop computer.
-
Internationalization: Our chatbot had built in language translation technology, creating an even better experience for folks
After identifying the best medium, we got to work on creating the bot flow (decision tree). This required daily reviews with the Ambulatory practice team, a group of project managers and clinicians advising us on changes to staffing (who would staff the live chat portion of our chat flow), updates from the telemedicine team (managing video visits and whether they could have patients directed to them), as well as rapidly changing guidance from the CIty of New York and the CDC around COVID symptoms. Over the course of 2 months, we made changes everyday around: symptoms triage, resolution endpoints, chatbot behaviors.

Click on any part to zoom.
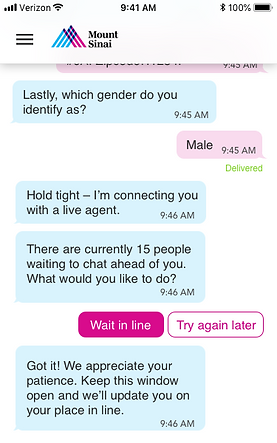
Case study in adaptation: Queuing
After about 1 week of launching our COVID-19 chat flow, we were quickly informed by the Patient Access Services team that their staff was getting crushed under the weight of incoming chat messages with the added complexity that staffing couldn’t scale up or down on the turn of a dime. If 500 people wrote in at noon, there were still only 10 nurses on staff, just the same as if 100 people wrote in at 9PM. On the patient side, there was no indication of a “waiting state,” so a lot of our initial reports that I reviewed saw a steep rate of abandonment during the connection between stepping up to livechat and actually connecting to an agent.
We solved this by creating a dynamic waiting queue based on the number of nurses logged into the chat platform, so that position in line represented was accurate. This queue was designed to ensure no one was ever waiting in line fruitlessly and was rather directed as quickly as possible to the best option the health system has to offer given capacity.
THe Results
At the peak of the COVID crisis in NYC, our chatbot was fielding an average of 150 unique entries to our chatbot, with 50 stepping up to speak with a nurse a day. We were able to offset, 800 were diverted to a video visit rather than one of our physical hospitals.
Sample EOW report

From Epic reporting, we learned that we helped drive a 700% increase in video visit traffic, contributing to lighter hospital visit loads.

The COVID-19 chatbot remains in place as we speak though the volume is understandably considerably down given that NYC has done an amazing job getting the virus under control. With a bit of breathing room, our team is now looking towards the Fall, when COVID will likely get worse again, to this MVP and make significant experience improvements, both to the service (having a dedicated COVID chat response team) and the platform (better accessibility across mobile and desktop, plus added internationalization).